

What Color Tube Do You Use To Draw Total Protein Labs
Fluid Analysis – Part 4 – Ascitic fluid, Peritoneal tap, abdominal paracentesis, abdominal tap procedure
Ascitic fluid
Sample
- The ascitic fluid is aspirated from the peritoneal crenel.
Definition of ascitic fluid
The collection of fluid in the peritoneal crenel is called ascites and is called ascitic fluid.
Indications
- An abdominal tap is done on the patient who has unexplained ascites.
- An intestinal tap is done to relieve the intraabdominal force per unit area.
- To diagnose whether ascites are benign or due to malignancy.
- An intestinal tap is helpful to differentiate between the medical or surgical belly.
- Abdominal fluid differentiates between Transudate or Exudate.
- The abdominal fluid is removed for diagnostic and therapeutic purposes.
Pathophysiology of ascitic fluid
- The peritoneal cavity is divers as the space between the visceral and parietal peritoneum.
- The fluid is constantly produced past the peritoneal membrane and also reabsorbed past the aforementioned membrane where they contain a network of capillary and lymphatics.
- If the secretion is increased or reabsorption is decreased that will lead to the collection of peritoneal fluid (Ascites).
- The abdominal fluid is classified as Transudate when protein is less than 3 G /dl or Exudate when poly peptide is more than 3 chiliad/dl.
- Transudate acquired by congestive middle failure, cirrhosis, nephrotic syndrome, myxedema, hypoproteinemia, peritoneal dialysis, and acute glomerulonephritis.
Exudate is constitute more commonly in inflammation and malignancy. While some other conditions of drug hypersensitivity, pulmonary infarction, GIT diseases, and collagen diseases may form exudate.
Procedure forascitic fluid tap:
- This is an invasive procedure.
- Ensure that the patient urinary bladder is empty.
- The position is semi-prone and lateral.
- Enhance the bedhead side so that fluid accumulates in the lower abdomen.
- Start, sterilize the area. Clean the area with 70% isopropanol and allow it to dry the area.
- If needed can give local anesthesia. Tin can raise the expanse with local coldhearted and make the small-scale bleb. from where the needle can be inserted.
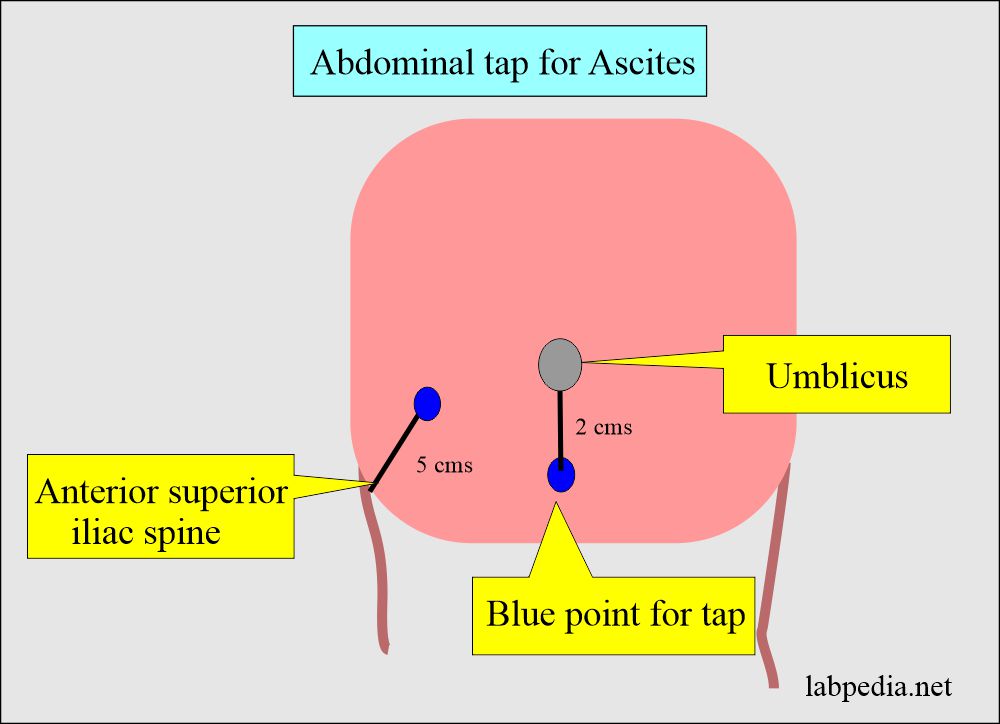
- Locate the surface area with percussion where there is dullness indicating fluid.
- Insert needle v cms superior and medial to the anterior superior iliac spine.
- Or ii cms below the umbilicus.
- A needle 20 or 18 judge is inserted into the abdominal cavity lateral to the umbilicus with constant negative pressure in the syringe, till you see the fluid.
Procedure for ascites tap
Complications of ascitic fluid tap
- There may be hypovolemia if a large volume of the ascitic fluid is aspirated.
- There is a hazard of peritonitis.
Normal features of ascitic fluid
| Characteristics | Findings |
| Colour | Articulate and light yellowish |
| Quantity | <fifty ml |
| Crimson blood cells | Nil |
| White blood cells | <300/cmm |
| Glucose | lxx to 100 mg/dL |
| Poly peptide | <iv.ane chiliad/dL |
| Amylase | 138 to 404 units/L |
| Alkaline phosphatase | Adult male = 90 to 240 units/L Adult female = 87 to 250 units/L |
| Lactate dehydrogenase (LDH) | Like serum level |
| Microscopic examination | Cytology = no malignant cells No bacteria No fungal bodies |
| Carcinoembryonic antigen (CEA) | Negative |
The Ascites, ( peritoneal fluid) analysis includes:
- Gross or physical appearance:
- Grossly peritoneal fluid is articulate, and low-cal yellow with <50 ml volume.
- No RBCs are seen.
- White blood cells are <300 /cmm
- Transudate fluid will be clear and straw color.
- Chylous color fluid: This is seen in blocked lymphatic vessels and the color is milky.
- This may be seen in lymphoma, carcinoma, and tuberculosis.
- In such fluids, triglyceride value is > 110 mg/dl.
- The inflammatory condition gives rise to a turbid or opaque color. This may be seen in with peritonitis, pancreatitis, and appendicitis.
- The hemorrhagic color is due to trauma or intraabdominal haemorrhage, tumor infiltrates, or hemorrhagic pancreatitis.
- Greenish color or bile-stained fluid is seen in the ruptured gallbladder, acute pancreatitis, or in abdominal perforation.
- Encarmine fluid may be due to:
- Traumatic tap.
- Hemorrhagic pancreatitis.
- Tumors.
- 10,000 RBCs/ µL will requite pink colour.
- xx,000 RBCs/ µL volition give encarmine appearance.
- Grossly peritoneal fluid is articulate, and low-cal yellow with <50 ml volume.
- Specific gravity: Exudate has a specific gravity of more than than 1.015 and less than ane.015 in transudate.
- Proteins: Transudate has less than iii g/dl and exudate has more than 3 g/dl of protein.
- The ratio of serum protein and ascitic fluid protein is more significant to differentiate exudate from transudate (Fluid poly peptide/serum protein).
- A ratio of more than 0.v is diagnostic of exudate.
- The albumin gradient between serum albumin and the ascitic fluid is besides important to differentiate between exudate and transudate.
- Ascitic fluid albumin -(minus) serum albumin.
- A value i.1 g/dL or more than indicates transudate.
- Value <1.1 g/dL indicates exudate.
- Ascitic fluid albumin -(minus) serum albumin.
- The ratio of serum protein and ascitic fluid protein is more significant to differentiate exudate from transudate (Fluid poly peptide/serum protein).
- Total Jail cell Count: This depends upon the cause of ascites.
- In the inflammatory conditions count volition exist high and predominantly Polys are seen.
- In hemorrhagic conditions, theRBC count will exist high.
- Differential count: The inflammatory weather evidence more polys and reactive mesothelial cells while transudate may bear witness more lymphocytes. Malignant ascites also show more than lymphocytes.
- RBCs presence indicates malignancies, tuberculosis, or intra-abdominal haemorrhage.
- WBCs presence indicates peritonitis, tuberculosis, or cirrhosis.
- Cytology: This can be done better on cytospin and can differentiate the cells and as well observe the malignant cells.
- Sometimes reactive mesothelial cells and malignant prison cell differentiation is difficult.
- Malignant cells take the variable morphology of the cells and nuclei. There is chromatin clumping and changed the nuclear/cytoplasmic ratio. May see prominent nucleoli.
- Glucose: level may be done which usually equal to blood glucose level.
- Simply in tuberculous and bacterial ascites is low.
- It is low in peritoneal carcinomatosis.
- Amylase: This will be raised in:
- Pancreatic trauma.
- Acute pancreatitis.
- Intestinal necrosis.
- Abdominal Perforation or strangulation.
- Pancreatic pseudocyst.
- Lactate dehydrogenase, (LDH): This is diagnostic for exudate if the ascites LDH/serum LDH ratio is greater than 0.6.
- The alkaline phosphatase level is greatly increased in infarction or the strangulation of the intestine.
- Ammonia raised level is seen in:
- Ruptured or strangulated intestine.
- Ruptured appendix.
- Gram stain: This may be performed but ordinarily culture and sensitivity are advised.
- Fungal infection usually is seen with histoplasmosis, candidiasis, or coccidioidomycosis.
- Carcinoembryonic antigen is seen in the case of GIT malignancies.
Interpretation of ascitic fluid:
| Physical appearance | Significance |
| Clear and pale yellow | Normal |
| Turbid | Bacterial infection |
| Bloodstained | Trauma, malignancy, or infection |
| Light-green | Gallbladder and pancreatic diseases |
| Milky | Lymphatic blockage and trauma |
| Biochemical findings | |
| Amylase | Pancreatitis and gastrointestinal perforation |
| Glucose | Decreased in TB peritonitis and malignancy |
| Alkaline phosphatase | Increased in gastrointestinal perforation |
| CEA | In malignancy of the gastrointestinal system |
| CA 125 | In ovarian malignancies |
| Blood urea nitrogen/creatinine | Ruptured and punctured urinary bladder |
| Microscopic findings | |
| WBCs count <500/cmm | Normal |
| >500/cmm | Bacterial peritonitis and cirrhosis |
| Gram stain and civilisation | Bacterial peritonitis |
| Acid-fast stain | TB peritonitis |
Differentiation of exudate and transudate:
| characteristics | Exudate | Transudate |
|---|---|---|
| appearance | cloudy/turbid | Clear / xanthous |
| Full poly peptide | > 3 G/dl | < 3 G/dl |
| ascitic protein/serum protein | > 0.five | < 0.5 |
| Specific gravity | > ane.015 | < 1.015 |
| Jail cell differential | Neutrophils | mononuclear cells |
| Glucose | < threescore mg/dl | equal to serum |
| LDH ascites / LDH serum | > 0.half dozen | < 0.half dozen |
| Fibrinogen | Clots | No clots |

Fluid exudate/transudate
- Note: Please see more details in fluid analysis function 2.
Go Dorsum to Fluid analysis
Comments

What Color Tube Do You Use To Draw Total Protein Labs,
Source: https://labpedia.net/fluid-analysis-part-4-ascitic-fluid-peritoneal-tap-abdominal-paracentesis-abdominal-tap-procedure/
Posted by: felixforridgen.blogspot.com
0 Response to "What Color Tube Do You Use To Draw Total Protein Labs"
Post a Comment